


We Specialize in Cardiac Rhythm Disorders


Dr. Rachita Navara, FACC, FHRS
Dr. Rachita Navara is a triple-board certified heart rhythm cardiologist trained at top institutions including UCSF (the birthplace of catheter ablation for arrhythmias), Stanford Medicine, Washington University in St. Louis, and University of Texas Southwestern Medical Center. With a strong background in both electrophysiology and bioengineering, she possesses a unique set of skills that allow her to offer a wide range of advanced procedures and treatments to her patients.
Dr. Navara serves as supervising physician for a Medicare-approved Independent Diagnostic Treatment Facility (IDTF) that enables participating physicians to perform and collect for studies for remote cardiac monitoring devices (e.g. Holters, Loop Recorders, Event Monitors, Mobile Cardiac Telemetry).
TREATMENTS

Transesophageal Echocardiograms
The procedure starts with the patient being administered a mild sedative to help them relax. An anesthetic is also applied to the throat to prevent discomfort. The patient is then asked to swallow a thin, flexible tube (the probe) which is gently guided down the esophagus.
The ultrasound device at the end of the probe sends sound waves that bounce off the heart, creating detailed images of the heart’s structures and allowing the physician to assess the size, shape, and movement of the heart’s walls and valves, as well as the flow of blood through the heart.
The TEE can provide valuable information about the presence of diseases or conditions such as heart valve disease, blood clots, or other abnormalities. The procedure typically takes between 30 minutes to an hour, and the patient is closely monitored throughout for any signs of discomfort or complications.
After the procedure, the patient may experience a mild sore throat, which usually resolves within a few hours. The sedative effects may also take a few hours to wear off, during which time the patient is advised to rest and avoid activities such as driving.

SVT (Atrial Flutter, AVNRT, AVRT, AT)
1. Atrial Flutter: This condition involves a rapid, regular rhythm in the atria caused by a “circuit” in the right atrium. The heart beats at a faster pace than normal, often ranging from 240 to 400 beats per minute.
2. AVNRT: This is the most common type of SVT and is caused by an extra pathway in the AV node that causes a reentry circuit, leading to rapid heart rates of 150-250 beats per minute.
3. AVRT: This is often associated with Wolff-Parkinson-White syndrome and involves an extra pathway outside the AV node. This additional pathway allows electrical impulses to bypass the AV node and move from the atria to the ventricles faster than usual, causing rapid heart rates.
4. AT: This involves abnormal electrical activity in the atria that causes the heart to beat rapidly and irregularly
Management of these conditions typically involves medications to slow the heart rate or convert the rhythm back to normal. In some cases, cardioversion (applying an electric shock to the heart) may be used.
If medications or cardioversion are not effective or suitable, a procedure called catheter ablation may be performed. This involves inserting a catheter into a vein, usually in the groin, and guiding it to the heart. Radiofrequency energy is then used to destroy the area of heart tissue causing the abnormal heart rhythm. This procedure has a high success rate and is typically safe, although there are potential risks which should be discussed with the healthcare provider.
Pericardiocentesis
The procedure is typically performed in a hospital under local anesthesia, although sedation may be used depending on the patient’s condition. The patient is placed on their back and connected to an electrocardiogram (ECG) machine to monitor heart activity throughout the procedure.
Under sterile conditions, the doctor inserts a needle into the chest wall, usually at the left or right of the sternum or below the xiphoid process. Using echocardiography or fluoroscopy as a guide, the needle is carefully advanced into the pericardial sac. A syringe is then attached to the needle to draw out the excess fluid.
Once the fluid is removed, a catheter may be left in place if continuous drainage is necessary. The needle insertion site is then bandaged. The removed fluid is often sent to a laboratory for analysis to determine the cause of the effusion.
The procedure usually takes about 20-60 minutes. After the procedure, the patient is closely monitored for several hours to ensure there are no complications.
Pericardiocentesis can provide immediate relief from symptoms associated with pericardial effusion such as shortness of breath, chest pain, or discomfort. This procedure also provides diagnostic information that can help determine the underlying cause of the effusion. As with all medical procedures, pericardiocentesis carries some risks, such as infection or puncture of the heart or lung, which should be discussed with the healthcare provider.

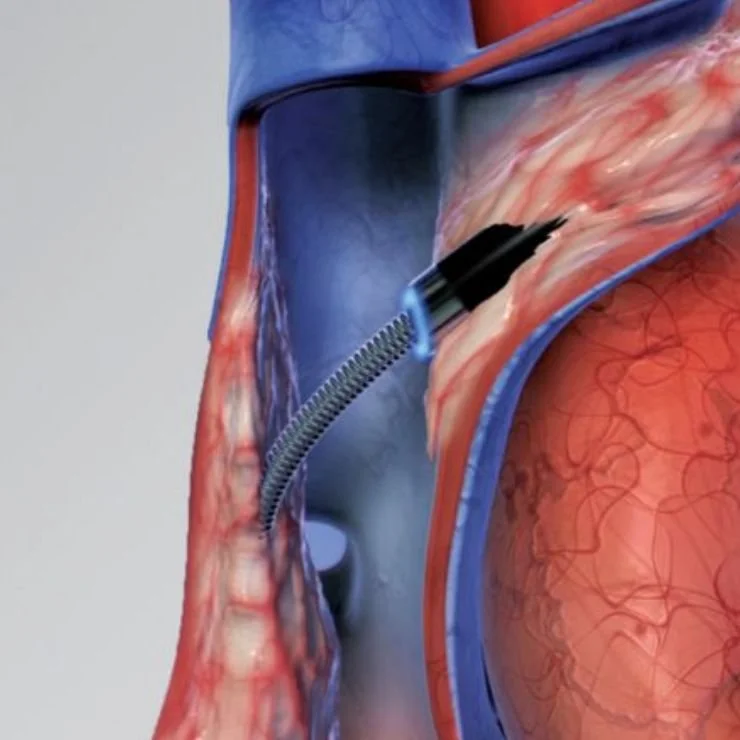
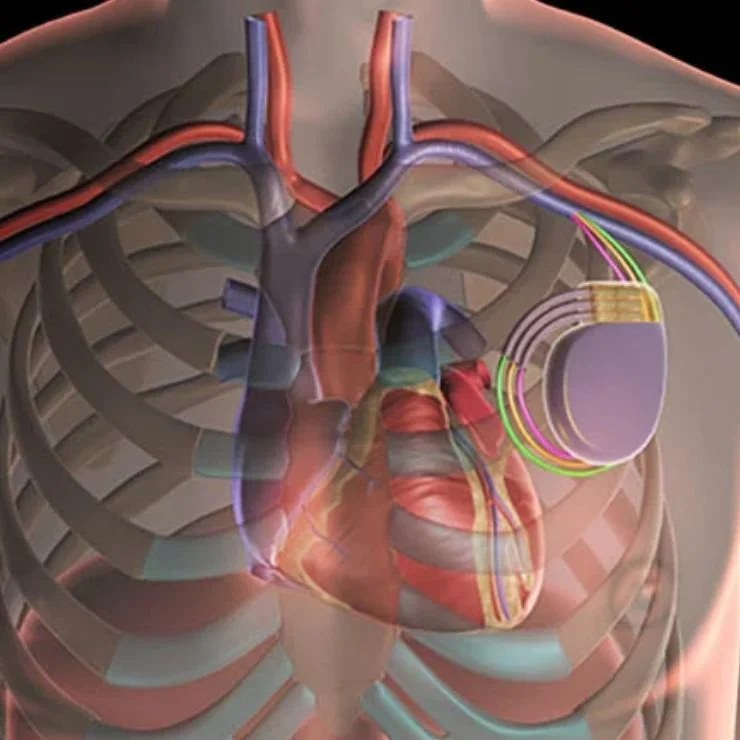
Leadless Pacemaker Implantation
1. Patient Preparation: The patient is positioned and local anesthesia is applied to the groin area to ensure comfort and prevent pain during the procedure. Continuous monitoring of the patient’s vital signs is maintained throughout.
2. Venous Access: The physician makes a small incision in the patient’s groin area to access the femoral vein.
3. Introduction of the Delivery Catheter: A specialized delivery catheter, containing the leadless pacemaker, is then introduced into the femoral vein.
4. Guided Placement: Using fluoroscopic imaging, the catheter is carefully navigated through the venous system and into the right ventricle of the heart.
5. Implantation: The leadless pacemaker is then deployed from the catheter. It attaches to the heart muscle with small tines and begins to monitor and regulate the heart’s rhythm.
6. Catheter Removal: Once the pacemaker is securely in place and functioning properly, the catheter is retracted and removed from the femoral vein.
7. Incision Closure: The incision in the groin is then sutured and bandaged.
8. Post-Procedure Monitoring: Following the procedure, the patient’s condition and the functioning of the pacemaker are closely monitored. The patient may be required to stay in the hospital overnight for observation.
9. Follow-Up Care: Regular follow-up visits will be scheduled to ensure the pacemaker is working correctly and the patient’s heart rhythm is effectively regulated.
10. Benefits: The leadless pacemaker implantation procedure is less invasive than traditional pacemaker surgery, resulting in reduced infection risks, no visible surgical scar, and quicker recovery times.

Implantable Loop Recorder Insertion/Explantation
The insertion procedure is relatively quick and minimally invasive. The patient is usually given local anesthesia to numb the area where the ILR will be inserted – typically in the left side of the chest, just beneath the skin. The physician makes a small incision, creates a pocket under the skin, and places the ILR in this pocket. The incision is then closed with sutures or adhesive, and a dressing is applied. The ILR is programmed to record abnormal heart rhythms automatically, but patients can also manually activate it if they experience symptoms.
The explantation, or removal, of the ILR is also a minor procedure. Local anesthesia is administered to numb the area, and a small incision is made over the site of the ILR. The physician carefully removes the device and then closes the incision.
Both procedures are typically performed on an outpatient basis, meaning the patient can go home the same day. After the insertion of an ILR, patients are instructed on how to monitor and report their symptoms. The device allows physicians to analyze the recorded data remotely, assisting in diagnosing heart rhythm abnormalities and guiding treatment decisions.
After explantation, the incision site is monitored for any signs of infection or complications. Regular follow-up appointments are scheduled to ensure the patient’s wellbeing.
This device can significantly improve the quality of life and survival rates for individuals with certain types of heart conditions. However, it’s important to discuss the benefits and potential risks with the healthcare provider before proceeding with ICD implantation.
Epicardial Mapping/Ablation
The procedure begins with the patient under general anesthesia. The surgeon then performs a minimally invasive procedure, often using a subxiphoid puncture or video-assisted thoracoscopy to access the pericardial space, the area surrounding the heart.
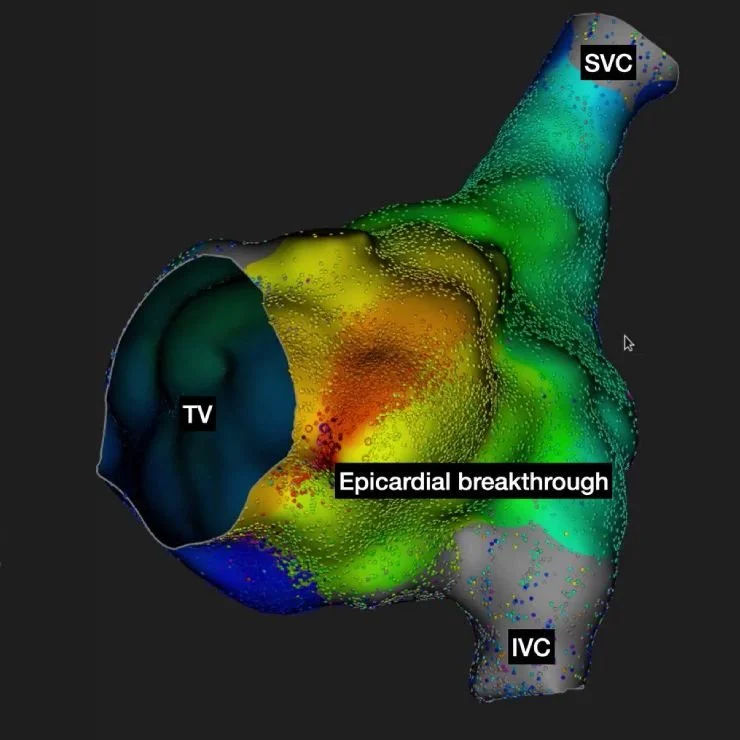
Once access is achieved, the surgeon uses a special catheter with an electrode at its tip to create a detailed map of the heart’s electrical activity, a process known as epicardial mapping. This map helps identify the precise location of the abnormal heart tissue causing the arrhythmia.
After the problem area is identified, the surgeon then performs the ablation. This involves delivering targeted energy (usually radiofrequency or cryoenergy) through the catheter to the abnormal heart tissue. This energy creates a small scar, which disrupts the irregular electrical signals, thereby correcting the arrhythmia.
Epicardial Mapping and Ablation is a complex procedure that requires a high level of expertise. While it carries risks such as bleeding, infection, and potential damage to surrounding heart tissue, it is a valuable tool in the treatment of complex arrhythmias that are not responsive to medication or less invasive procedures.
Post-procedure, patients are closely monitored in the hospital for a few days, and follow-up appointments are scheduled to ensure the heart is functioning correctly. Patients are also advised to report any unusual symptoms to their healthcare provider immediately
Cardioversions
The procedure is usually performed in a hospital or specialized clinic, where the patient’s heart activity can be closely monitored. It’s typically a scheduled procedure, but in emergencies, it may be done urgently to stabilize a patient’s condition. Prior to the procedure, the patient is often sedated to help them remain comfortable and calm.
The following are the advantages: 1. Restores Normal Heart Rhythm: The primary advantage of cardioversion is that it can restore a normal heart rhythm in patients with certain types of abnormal heartbeats, particularly atrial fibrillation or atrial flutter.
2. Immediate Results: Cardioversion often works immediately, allowing patients to return to their regular daily activities without delay.
3. Non-Invasive Procedure: Cardioversion is a non-invasive procedure that involves delivering a brief electric shock to the heart, which can help reset the heart’s electrical activity.
4. Controlled Environment: The procedure is performed in a controlled medical environment, under supervision of medical experts. This ensures safety and immediate medical attention if required.
5. Prevents Complications: By restoring normal heart rhythm, cardioversion can help prevent serious complications that can arise from untreated arrhythmias, such as stroke or heart failure.
6. Symptom Relief: For patients suffering from symptoms such as palpitations, shortness of breath, or fatigue due to their arrhythmia, cardioversion can provide significant symptom relief.
7. Short Procedure Time: Cardioversion is a relatively quick procedure, often completed within a few hours, including preparation and recovery time.
8. Option for Drug-Resistant Cases: For patients whose arrhythmias are not controlled by medication, cardioversion can be a viable alternative treatment option.
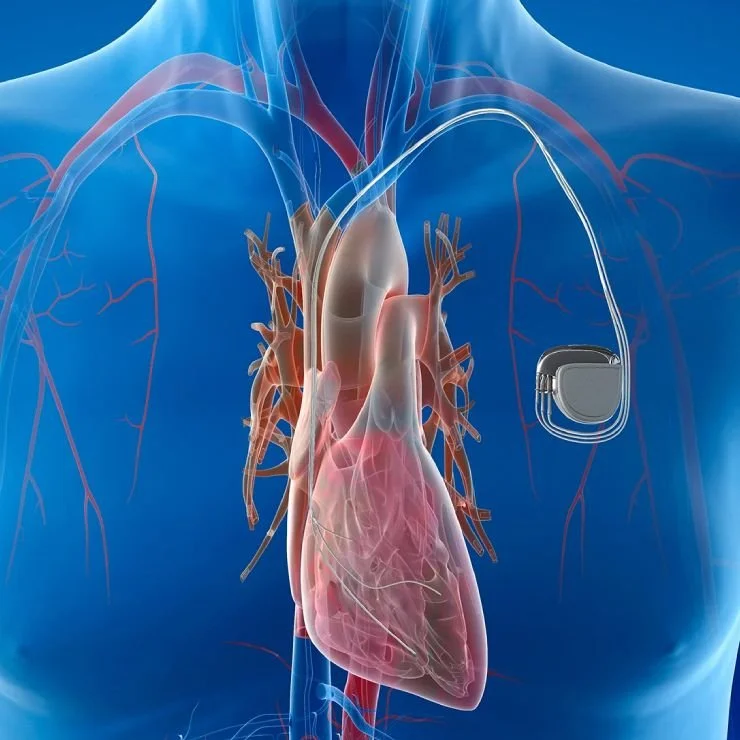
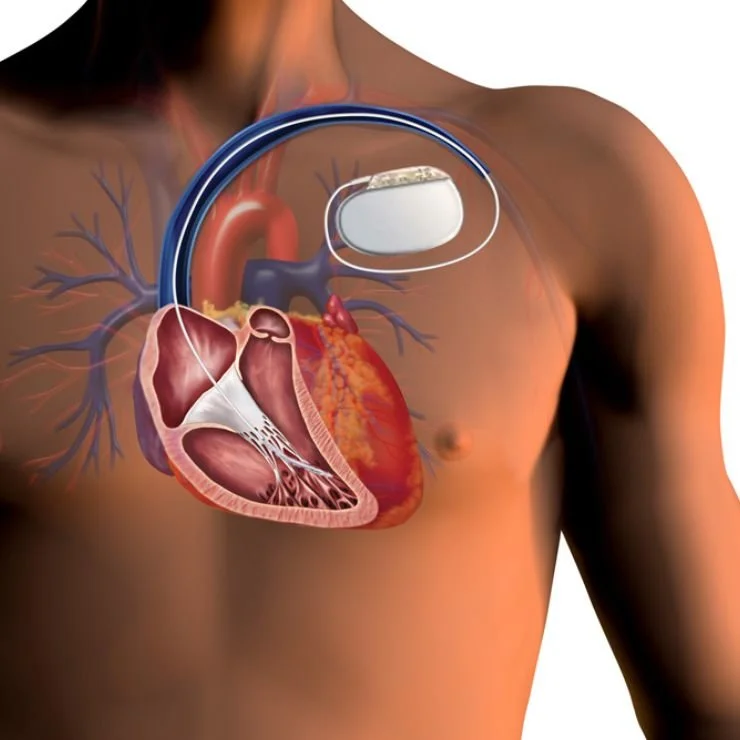
Pacemakers
The procedure typically begins with the administration of a local anesthetic to numb the area where the pacemaker will be inserted, usually in the upper chest. The physician then makes a small incision in the chest and inserts a lead (a flexible, insulated wire) into a vein. This lead is guided through the vein, using real-time imaging technology, until it reaches the heart.
The lead has an electrode at its tip, which will deliver the electrical impulses from the pacemaker to the heart. Once the lead is in the correct position, the other end is connected to the pacemaker device. The pacemaker is then inserted into a small pocket created by the physician under the skin in the chest.
The whole procedure usually takes about one to two hours. After the procedure, the pacemaker’s settings can be adjusted as necessary to ensure the heart is beating at the right pace. The patient’s heart rhythm and the function of the pacemaker are regularly monitored to ensure it is working correctly.

Stress Echocardiograms
The procedure begins with a resting echocardiogram where images of the heart are taken while the patient is at rest to provide a baseline for comparison. Electrodes are attached to the patient’s chest to monitor their heart rate and rhythm.
Once the resting images are taken, the stress test begins. The patient is asked to exercise on a treadmill or stationary bicycle to increase their heart rate. If the patient is unable to exercise, a medication may be administered to mimic the effects of exercise on the heart.
When the patient’s heart rate reaches a target level, or if the patient starts experiencing symptoms such as chest discomfort or breathlessness, another set of echocardiogram images is taken. These images are then compared with the resting images to assess any changes in the heart’s function.
The Stress Echocardiogram helps the physician to diagnose and evaluate a range of heart conditions, such as coronary artery disease, heart valve disease, or heart failure. It can also help the physician to determine the patient’s exercise tolerance and to formulate a suitable exercise program.
The procedure typically takes between 45 minutes to an hour. After the test, the patient may feel tired, but should be able to resume normal activities unless advised otherwise by the physician.
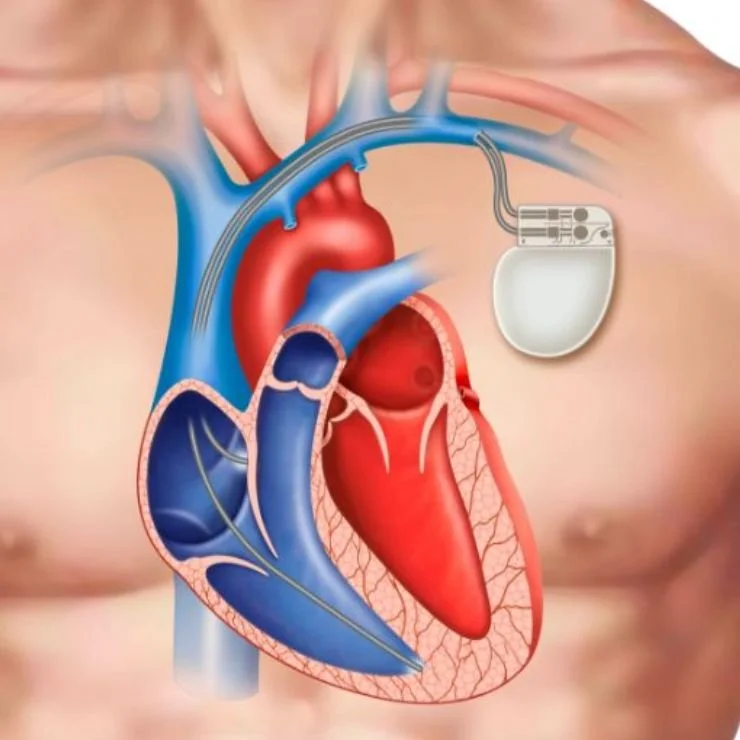
Generator Change
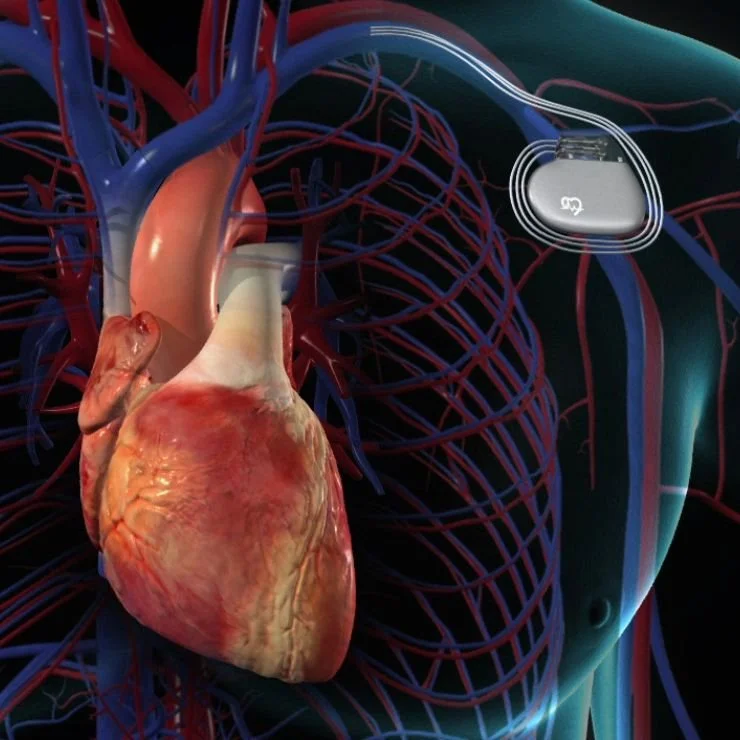
Pacemakers and ICDs are small, battery-operated devices implanted under the skin near the heart to monitor and regulate abnormal heart rhythms. Dualchamber (DDD) pacemakers are a specific type of pacemaker that control the timing and sequence of the heart’s two upper and two lower chambers to ensure they are working together effectively.
Over time, the battery life of these devices diminishes and requires replacement – typically every 5 to 15 years, depending on the device and how often it is used. Additionally, leads may need to be adjusted, replaced, or removed due to breakage, dislodgement, or infection.
The procedure is performed under local anesthesia with mild sedation. The surgeon makes a small incision over the site of the existing device. The old generator is disconnected from the leads and removed, and a new generator is connected and placed back into the pocket under the skin. If a lead needs to be replaced, the old lead might be removed, and a new one is threaded through the blood vessels to the heart.
After the procedure, the patient may need to stay in the hospital for a day or so for monitoring. Regular follow-up appointments will be necessary to ensure the device’s function and make any necessary adjustments.
While generally considered safe, the procedure does carry potential risks, including infection, bleeding, bruising, damage to blood vessels or nerves, and rarely, puncture of the heart.
As with any medical procedure, it’s essential for patients to discuss the benefits and potential risks with their healthcare provider before proceeding. The decision to have a Pacemaker/ICD revision or ICD generator change depends on the patient’s overall health, the type of device, the condition of the leads, and the specific heart condition being treated.
Cardiac Device Interrogations
During a pacemaker interrogation, the healthcare provider uses a specialized computer, called a programmer, which communicates with the pacemaker through a wand placed over the skin where the device is implanted. This process is entirely painless and typically takes between 15 and 30 minutes.
The interrogation allows the healthcare provider to assess various aspects of the pacemaker’s performance, including battery life, lead impedance, heart rhythm, and any recorded arrhythmias. It also reveals how often the pacemaker is being used and can help identify if the device or leads are malfunctioning.
The data collected from the interrogation is used to adjust the pacemaker settings if necessary, ensuring the device continues to work optimally for the patient’s specific needs. This could include adjustments to the pacing mode, rate, or voltage, among other parameters.
Pacemaker interrogations are typically performed at regular intervals, commonly every 3 to 12 months, but the frequency may vary based on the specific type of device, the patient’s medical condition, and the physician’s recommendation.
It’s important to note that while pacemaker interrogations provide valuable data on the device’s functioning, they do not replace routine medical check-ups with the healthcare provider. Regular follow-up appointments are still necessary to monitor the patient’s overall health and response to the pacemaker.
Atrial Fibrillation Ablation
The procedure is usually performed in a hospital’s electrophysiology (EP) lab. Patients may be given a general anesthetic or a sedative to ensure comfort throughout the procedure. The specialist, an electrophysiologist, will insert thin, flexible tubes called catheters into the patient’s blood vessels, typically in the groin, and guide them to the heart using real-time imaging, such as fluoroscopy.
Once the catheters are in place, the electrophysiologist will use one of two types of energy to create the scar tissue: radiofrequency energy, which uses heat, or cryoablation, which uses extreme cold. The choice of energy type is usually determined by the patient’s specific condition and the electrophysiologist’s preference.
The process of creating the scar tissue will block the abnormal electrical signals causing the atrial fibrillation, thereby restoring the heart’s normal rhythm. The entire procedure usually takes several hours, and most patients are able to go home the same day or the following day.
Post-procedure, patients are closely monitored to ensure the heart is maintaining a normal rhythm and to detect any potential complications. For some patients, medication or a pacemaker may still be required to help control heart rhythm.
Like any medical procedure, atrial fibrillation ablation carries some risk, including bleeding, infection, stroke, heart attack, or damage to the heart or blood vessels. All potential risks should be thoroughly discussed with the healthcare provider prior to the procedure.
Lead Extraction/ DDD Pacemaker Extraction
The procedure is typically performed under local anesthesia with sedation or general anesthesia. It begins with the surgeon making a small incision over the original pacemaker implantation site, usually in the upper chest.
Using specialized tools, the surgeon disconnects the pacemaker device from the leads. Following this, the leads are carefully extracted. This can be challenging as over time, the body’s natural response can cause tissue to grow over the leads, securing them in place. Special sheaths and laser technology may be used to safely free the leads without damaging the heart or blood vessels.
Once the leads and pacemaker are successfully removed, a new device and leads may be implanted if necessary, often at a different site. The incision is then closed and the area bandaged.
Lead extraction is considered a high-risk procedure and is typically performed when the leads or pacemaker are not functioning correctly, are infected, or are causing other complications.
After the procedure, patients are closely monitored in the hospital to ensure there are no complications. Recovery time varies depending on the individual patient’s health status and whether a new device was implanted. Patients are advised to avoid heavy lifting and vigorous physical activity for a period of time post-procedure and will have regular follow-up appointments to monitor their progress.
PVC/VT
1. PVCs: Premature Ventricular Contractions are extra, abnormal heartbeats that begin in the ventricles and disrupt the regular heart rhythm. PVCs may cause a sensation of a “flip-flop” or skipped beat in the chest. While they are usually harmless, frequent PVCs can sometimes lead to other rhythm problems or weak heart function if they occur frequently over a long period.
2. VT: Ventricular Tachycardia is a rapid heart rate that originates with abnormal electrical signals in the ventricles. The rapid heart rate prevents the ventricles from filling and contracting efficiently to pump enough blood to the body. VT can become life-threatening if it lasts for more than a few seconds.
The treatment of these conditions depends on their frequency, symptoms, and underlying cause. Medications may be used to control the heart rhythm or to treat any underlying heart disease. If medication is not effective, procedures like cardioversion (electric shocks to the heart) or catheter ablation (where a catheter is used to destroy the area of heart tissue causing the abnormal rhythm) may be recommended.
Another option for patients with life-threatening arrhythmias is the implantation of an Implantable Cardioverter Defibrillator (ICD). The ICD continuously monitors the heart rhythm and delivers precise electrical shocks to restore a normal rhythm when needed.
These procedures should always be discussed thoroughly with the healthcare provider to understand the potential benefits and risks.
LA Appendage Ligation
During the procedure, the surgeon accesses the heart through small incisions in the chest, often using a video-assisted thoracoscope or a robotic surgical system for better visibility and precision. The left atrial appendage is then identified, and a special device or suture is used to seal off or “ligate” the appendage. This prevents the blood from entering and clotting in the appendage, thereby reducing the risk of stroke.
The procedure can be performed as a standalone operation or in conjunction with other heart surgeries. It may be an alternative for patients who cannot tolerate long-term anticoagulation therapy.
Left Atrial Appendage Ligation is typically performed under general anesthesia and may require a hospital stay of a few days for monitoring and recovery. As with any surgical procedure, it carries certain risks, including bleeding, infection, and complications related to anesthesia. However, it can significantly reduce the risk of stroke in patients with atrial fibrillation, improving their quality of life.
Post-operatively, patients will require regular follow-up appointments to monitor their recovery and ensure the effectiveness of the ligation. It’s essential for patients to maintain communication with their healthcare providers and report any new or worsening symptoms promptly.
ICD Implant
The procedure is performed under local anesthesia, often with sedation for comfort. It involves the insertion of the ICD, a small electronic device about the size of a pocket watch, under the skin in the chest area. One or more flexible, insulated wires, known as leads, are inserted into veins and guided to the heart using X-ray imaging. The other ends of these leads are connected to the ICD.
The ICD continuously monitors the heart rhythm. In case of detection of an abnormal heart rhythm, it can deliver electrical pulses or shocks to restore a normal rhythm. It can also work as a pacemaker and speed up the heart if it’s beating too slowly.
ICD implantation is generally a safe procedure with a low risk of complications. However, potential risks can include infection at the implant site, bleeding, damage to blood vessels or nerves, and rarely, puncture of the heart.
Post procedure, patients are typically monitored overnight and can often return home the next day. Regular follow-ups are necessary to ensure the ICD is functioning correctly and to adjust settings if needed.
This device can significantly improve the quality of life and survival rates for individuals with certain types of heart conditions. However, it’s important to discuss the benefits and potential risks with the healthcare provider before proceeding with ICD implantation.
EP Study
The procedure is conducted in a special room called an electrophysiology lab under the supervision of a cardiologist specialized in electrophysiology. It involves inserting one or more thin, flexible tubes, called catheters, into a blood vessel (usually in the groin or neck) and guiding them to the heart with the help of X-ray imaging.
Once the catheters are in place, they are used to send small electrical impulses to the heart, which may induce the arrhythmia. This helps the doctor to analyze the spread of these impulses throughout the heart during each beat and locate the areas causing the rhythm problems.
The EP Study can provide essential information about the nature of the abnormal heart rhythm, which cannot be obtained from an ECG, a stress test, or any other non-invasive test. It can help determine whether the patient would benefit from treatments like medication, a pacemaker, an implantable cardioverter defibrillator (ICD), cardiac ablation, or surgery.
Although an EP Study is an invasive procedure, it is generally safe with a low risk of complications. However, as with any medical procedure, there may be potential risks which should be discussed with the healthcare provider before the procedure.
Biventricular Devices
The device works by coordinating the contractions between the heart’s two ventricles, ensuring they pump blood into the body more efficiently. It also incorporates a defibrillator function which can deliver a shock to the heart in case of life-threatening arrhythmias, thus providing an added layer of protection.
The procedure is performed under local anesthesia with mild sedation for patient comfort. The CRT-D device, which is similar in size to a small pocket watch, is implanted under the skin in the upper chest area. Insulated wires, known as leads, are inserted into veins and guided into the heart using X-ray imaging. These leads are connected to the device and are positioned in three areas of the heart: the right atrium, the right ventricle, and the left ventricle, hence the term “biventricular.”
The CRT-D device continuously monitors the heart rhythm and delivers small electrical impulses to stimulate and synchronize the heart chambers if they are beating out of sync. It also acts as an automatic defibrillator if dangerous heart rhythms are detected, delivering a shock to restore a normal rhythm.
While generally considered safe, the procedure does carry potential risks, including infection at the implant site, bleeding, damage to blood vessels or nerves, and rarely, puncture of the heart.
After the procedure, the patient may need to stay in the hospital for a day or so for monitoring. Regular follow-up appointments will be necessary to check the device’s function and make any necessary adjustments.
BiV or CRT-D implantation can significantly improve quality of life and survival rates for individuals with specific types of heart conditions. However, it’s essential for patients to discuss the benefits and potential risks with their healthcare provider before proceeding with implantation.
Atrial Flutter Ablation
The procedure is typically performed in a hospital’s electrophysiology (EP) lab. The patient is usually given a sedative or general anesthetic to ensure comfort throughout the procedure. The physician, an electrophysiologist, will insert thin, flexible tubes called catheters into a blood vessel, often in the groin, and guide them to the heart using real-time imaging techniques, such as fluoroscopy.
Once the catheters are correctly positioned, the electrophysiologist will deliver radiofrequency energy through the catheter to the area causing the atrial flutter. This energy creates a scar, effectively disrupting the abnormal electrical circuit and stopping the rapid, regular heartbeat.
The entire procedure typically takes two to four hours. Most patients can expect to go home the same day or the following day. After the procedure, patients are closely monitored to ensure that the heart is maintaining a normal rhythm and to detect any potential complications.
As with any medical procedure, there are potential risks associated with atrial flutter ablation, including bleeding, infection, stroke, heart attack, or damage to the heart or the surrounding blood vessels. These risks should be thoroughly discussed with the healthcare provider prior to the procedure. In some cases, medication or a pacemaker may still be required to help control heart rhythm.
Our Partners



